
Consistently High Patient Satisfaction
RMCC implements a widely used methodology known as the Net Promoter Score, which allows for the real-time evaluation of service quality and patient satisfaction. By industry standards, a score of 75 percent or above is considered high. Consistently scoring above 80 percent, RMCC ranks among the highest recorded in any industry.
Clinical Excellence With a Personal Touch
At RMCC, our search for new treatments is relentless. Our drive to provide superior care runs deep. And our fight against cancer is personal. Our independent, physician-led practice is known for delivering clinical excellence combined with unmatched personal and emotional support in neighborhoods through the front range.
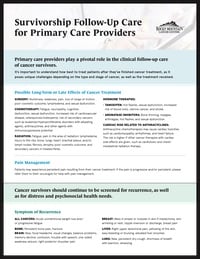
Survivorship Follow-Up Care for Primary Care Providers
It’s important to understand how best to treat patients after they’ve finished cancer treatment, as it poses unique challenges depending on the type and stage of cancer, as well as the treatment received.
Helpful Information for Referring Providers



-
Hematology Work-Up Refresher
-
Radiotherapy Updates for Oligometastases
-
Men's Oncology Health
-
Women's Health Oncology & Hematology
-
Managing the Side Effects of Your Patients on Active Cancer Treatment
-
The Transformational Year in Gastrointestinal Cancers
-
Breast Cancer Updates for the Primary Care Provider
-
Hematology Updates for the Primary Care Provider
-
Lung Cancer Screening, Diagnosis and Treatment for the Primary Care Provider
-
Colorectal Cancer Updates 2023
-
ASH Updates 2022
-
ASH Updates 2022
-
New Radiation Oncology Technologies for Diagnosis & Treatment of Common Cancers
-
ASH Updates 2021
-
Lung Cancer Update - Precision Medicine
-
Cancer Screening and Cancer Prevention
-
Genetic Risk Evaluation and Testing (GREAT) High Risk Program
-
RMCC Lymphedema Prevention Program
-
The Latest News in Colorectal Cancer
-
Hypofractionated Radiation
-
Understanding Your Breast Cancer Pathology Report
-
Genomic Assays and Breast Cancer
-
Metastatic Prostate Cancer Research Updates
-
Adjuvant Endocrine Therapy for Breast Cancer
-
Advances in the Treatment of Non-Hodgkin Lymphoma
-
Introduction to Chronic Lymphocytic Leukemia
-
Prostate Cancer Radiation Explanations to Support Informed Decisions
-
Metastatic Hormone Positive Breast Cancer
-
Topics in Breast Cancer Surgery
-
ASH Updates 2020: Lymphoma and CLL
-
ASCO Updates 2020: Colon Cancer
-
ASCO Updates 2020: Bladder Cancer
-
ASCO Updates 2020: Blood Cancers
-
ASCO Updates 2020: Breast Cancer
-
ASCO Updates 2020: Lung Cancer